干眼症和白内障都是常见的老年性眼病。事实上,这类眼病经常同时发生,而且会在一些重要方面相互影响。1如果您正准备接受白内障手术,了解干眼症与手术效果之间的联系是帮助您在术后获得理想视力效果的关键。
什么是干眼症?
随着年龄的增长,我们眼睛分泌的泪液越来越少,质量也越来越差,无法为眼睛带来足够的润滑作用。这会损害眼睛表面或角膜,导致炎症和以下症状:2
- 眼睛有烧灼感、刺痛感或搔痒感
- 视力模糊,眨眼后有所改善
- 就像眼睛里有沙子的含沙砾感
- 眼睛发红或眼睛内部或周围有成丝状粘液
- 眼睛流泪
- 眼睛疲劳
- 对光线敏感
- 佩戴隐形眼镜困难
- 夜间驾驶困难
果您怀疑自己患有干眼症或出现任何相关症状,请务必在接受白内障手术前与您的眼科医疗服务提供者进行沟通。在手术前的评估中,您的服务提供者会询问您的干眼症状,并进行临床评估,检查是否有干眼症的迹象。这一步至关重要,因为有些患者可能感觉不到任何症状,但仍有潜在的干眼症临床表现,只有通过适当的检查才能发现。如果患有干眼症,在手术前启动治疗方案非常重要,因为提前控制病情可以改善手术效果和整体舒适度。
白内障手术如何影响干眼症
白内障手术是安全有效的,但它可能会暂时加重您原有的干眼症状,或带来新的干眼症状。这是由于手术破坏了眼球表面、白内障手术过程中手术显微镜发出的强光以及白内障手术后使用的处方药(如类固醇和抗生素眼药水)造成的。3-6这些都可能导致泪液分泌的暂时性改变,但通常会随着时间的推移和适当的护理而得到改善。7如果干眼症状得不到控制,就会影响伤口愈合和视觉清晰度。
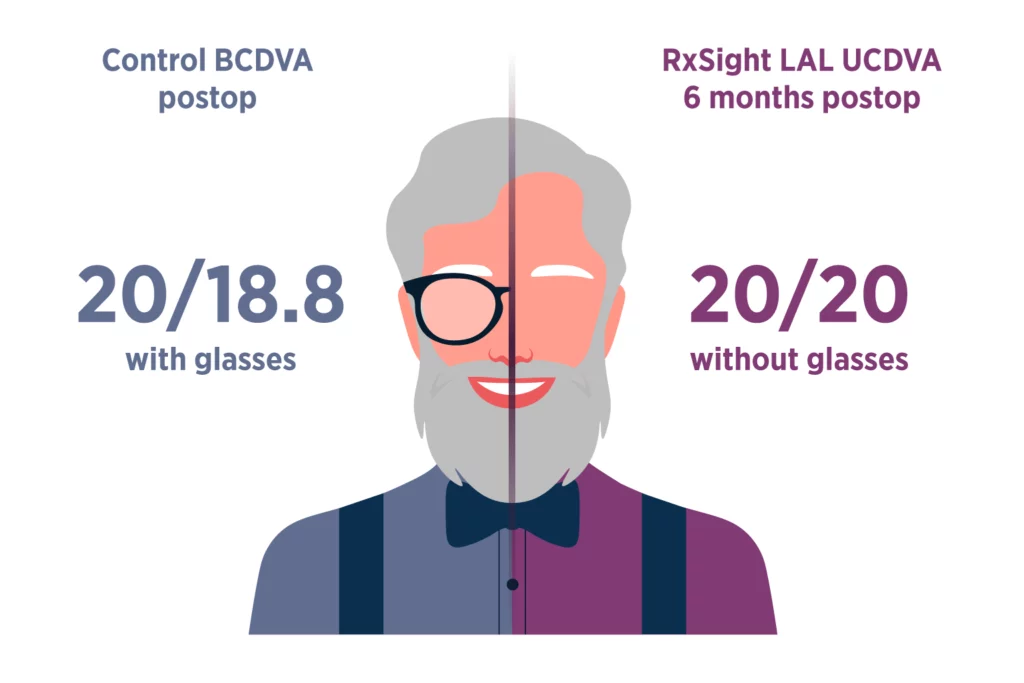
健康的泪膜对清晰的视力至关重要。当眼球表面干燥或受到刺激时,光线在到达视网膜之前就会散射,从而降低图像质量,使术后调整的测量工作变得困难。为了帮助确保任何人工晶状体(包括 RxSight Light Adjustable Lens™ (LAL™))都能获得清晰的图像质量,在手术前后可能需要进行干眼症治疗,以便让您的眼球表面有时间在手术后恢复。此外,让您的眼球表面处于最佳状态对于精确光照调整也非常重要。
术后保护眼睛健康
使用 LAL 进行白内障手术后,您将经历三个阶段的护理,包括术后恢复期、视力个性化调整期以及最终锁定期。以下是每个阶段的主要注意事项:
术后恢复期。 术后恢复期。术后几天内,视力模糊或朦胧,感觉轻微刺激是正常的。这是恢复过程的一部分。除了使用 RxSight 防紫外线眼镜外,还必须遵照眼科护理团队提供的眼药水使用说明,以优化眼睛恢复。其中包括用于预防感染和促进恢复的处方眼药水,以及用于维持眼表健康的人工泪液。
视力个性化调整期。 当您和眼科医生一起努力将视力调整到您喜欢的程度时,一定要在整个光照调整过程中坚持使用眼药水,以促进眼表健康。
最终锁定期。 一旦您对自己的视力感到满意,现在就是锁定晶状体度数的时候了。为了达到最佳效果,尽可能保持眼表健康非常重要。
为了在白内障手术后和整个光照调整过程中尽量减少干眼症状,促进眼表健康,请遵守以下建议:
- 遵照眼科医生的指示在术后滴眼药水。 这些眼药水可以减轻炎症、预防感染并保持眼球表面健康。
- 遵医嘱使用人工泪液。
- 在恢复初期,避免过多看电子产品,因为这会减少眨眼次数。
- 如果持续感到不适,及时向外科医生报告。
要旨
干眼症和白内障常有连带关系,但只要在手术前后进行适当的护理,就能保护您的舒适度、视力和眼睛的长期健康。如果您选择了 RxSight Light Adjustable Lens(光可调晶状体),保持眼睛健康将有助于您获得最清晰、最精确的效果。
- Donthineni PR, Deshmukh R, Ramamurthy C, et al. Management of cataract in dry eye disease: preferred practice pattern guidelines. In J Ophthalmol. 2023;71(4):1364-1372.
- Mayo Clinic. Dry eyes. Accessed August 14, 2025. https://www.mayoclinic.org/diseases-conditions/dry-eyes/symptoms-causes/syc-20371863
- Ishrat S, Nema N, Chandravanshi SCL. Incidence and pattern of dry eye after cataract surgery. Saudi J Ophthalmol. 2018;33(10):34-40.
- Sutu C, Fukuoka H, Afshari NA Mechanisms and management of dry eye in cataract surgery patients. Curr Opin Ophthalmol. 2016;27:24-30.
- Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol. 2009;23:65-73.
- Li XM, Hu L, Hu J, Wang W. Investigation of dry eye disease and analysis of the pathogenic factors in patients after cataract surgery. Cornea. 2007;26(9 Suppl 1):S16-S20.
- Yao K, Bao Y, Ye J. Efficacy of 1% carboxymethylcellulose sodium for treating dry eye after phacoemulsification results from a multicenter, open-label, randomized, controlled study. BMC Ophthalmol. 2015;15:28.