The Light Adjustable Lens™ (LAL®) is the first and only FDA-approved intraocular lens (IOL) that can be customized after cataract surgery—and when surgeons face that decision themselves, it’s the lens they choose. That says everything.
An IOL Surgeons Trust for Their Own Eyes
Unlike standard IOLs—set to a fixed power before the eye has fully healed—the LAL can be fine-tuned postoperatively through a series of brief, non-invasive light treatments. For surgeons who’ve spent careers working around the limitations of fixed optics, that distinction matters.
If you’re evaluating the LAL for your practice, contact us for more information to help you move forward.
The Light Adjustable Lens has transformed cataract surgery by shifting crucial decisions regarding final lens power to the more ideal post-surgery period. This approach allows for unparalleled precision, as it accounts for lens shift and refractive changes that can occur during the healing process to achieve the best possible outcomes.
The innovative Light Adjustable Lens represents a departure from the usual practice of selecting a pre-manufactured lens power before surgery to predict a patient’s post-surgery visual outcome. The accuracy of vision achieved with the postoperative adjustability of the Light Adjustable Lens compared to traditional premium IOLs has been demonstrated in clinical studies.
The Light Adjustable Lens corrects as low as 0.50 D of astigmatism, which is the lowest level approved to be treated.
How does the Light Adjustable Lens address residual astigmatism?
Residual astigmatism after cataract surgery is a common source of patient dissatisfaction with fixed IOLs. The LAL adjustment process allows cylinder correction postoperatively—after the eye has stabilized—rather than relying on preoperative biometry alone. For patients with complex refractive history or unpredictable measurements, the post-surgical adjustment window provides a precision mechanism that fixed lenses cannot offer.
The Light Adjustable Lens offers LASIK-like accuracy in cataract surgery.2,3
The Light Adjustable Lens provides optimized vision for patient satisfaction.2
Audrey Talley Rostov, MD
Light Adjustable Lens Patient
“Choosing the Light Adjustable Lens was one of the best decisions I’ve ever made.
Being able to wake up, see clearly, and enjoy activities like swimming, running, hiking, and traveling has been truly life-changing.
When patients learn that I trusted the LAL for my own eyes, it gives them confidence in their decision. After my surgery, I encouraged my father-in-law to have cataract surgery, and he chose the Light Adjustable Lens as well. Two years later, I’m still very happy with my vision.”
Paid consultant for RxSight. Views are their own.
Samir Melki, MD, PhD
Light Adjustable Lens Patient
“After seeing the results in my patients, choosing the Light Adjustable Lens was easy.
Seeing the outcomes in my own patients made choosing the Light Adjustable Lens an easy decision. What stood out to me personally was the value of being able to fine-tune the result rather than settling. My vision today feels as crisp as it did in my contact lens days. Having gone through it myself, I truly believe we will one day look back and wonder how we accepted non-adjustable lenses.”
Paid consultant for RxSight. Views are their own.
Jamie Monroe, MD
Light Adjustable Lens Patient
“My visual outcome has been outstanding.
I chose the Light Adjustable Lens after seeing the quality of vision my patients were achieving. Being able to test-drive my own vision and guide the decision-making process was incredibly valuable. That experience allows me to confidently tell colleagues and patients that it provides excellent visual quality with minimal compromise.”
Paid consultant for RxSight. Views are their own.
Andrew Caster, MD
Light Adjustable Lens Patient
“I appreciated being able to personalize my outcome.
As a refractive surgeon, visual quality and precision are my top priorities. I wanted the highest likelihood of achieving accurate, high-quality vision while minimizing residual refractive error, so the Light Adjustable Lens was a natural choice for me. The adjustment process was straightforward and comfortable, and I would make the same choice again.”
Paid consultant for RxSight. Views are their own.
Jeff Machat, MD
Light Adjustable Lens Patient
“For me, it came down to precision and adjustability.
When I was choosing my own lens, I asked several surgeons what they would select for themselves, and the overwhelming recommendation was the Light Adjustable Lens. As a surgeon, I understand the limitations of any procedure and how healing can influence the final result, so having the ability to adjust my vision after surgery was a major factor in my decision. That level of precision has left me very satisfied with my outcome.”
Paid consultant for RxSight. Views are their own.
Daniel Durrie, MD
Light Adjustable Lens Patient
“My outcome has been excellent and stable.
As a surgeon, I knew the options well and wanted the most precise, customizable approach available. The ability to experience my vision and refine it without rushing the process was incredibly valuable. Overall, it has been a very satisfying experience.”
Paid consultant for RxSight. Views are their own.
James Davies, MD
Light Adjustable Lens Patient
“Choosing the Light Adjustable Lens is one of the best decisions I have made.
I selected the Light Adjustable Lens for my own eyes because it removed uncertainty. Being able to refine my vision after surgery gave me confidence in the process, and today I simply do not think about my vision anymore. Having experienced it myself, I recommend it to patients with complete confidence.”
Paid consultant for RxSight. Views are their own.
Ronald Gaster, MD, FACS
Light Adjustable Lens Patient
“For me, these lenses have truly felt like a miracle.
As a surgeon, I understood the advantages of the Light Adjustable Lens for my own eyes. The ability to adjust and fine-tune my vision gave me tremendous confidence in the process. The extra postoperative time was absolutely worth it. It is remarkable to experience such stable, high-quality vision.”
Paid consultant for RxSight. Views are their own.
Alan Faulkner, MD
Light Adjustable Lens Patient
“The ability to experience my vision and then refine it made all the difference.
As surgeons, we know that predicting the exact refractive outcome isn’t always straightforward. Being able to adjust my vision based on real-world experience was incredibly valuable. That flexibility allowed me to land on an outcome that truly suited my visual needs, and I’m very pleased with the quality of my vision.”
Paid consultant for RxSight. Views are their own.
Adjust for Infinite Possibilities
The Light Adjustable Lens is a versatile premium lens that a growing number of surgeons are finding is customizable for many types of patients. Throughout the adjustment process, Light Adjustable Lens patients are engaged and participate in their care in a way other lenses can’t offer.
This truly customized approach has led to outcomes they and their doctors are excited about. Almost daily, we add to the list of clinics nationwide that are successfully integrating the Light Adjustable Lens into their workflow and finding that it is a worthwhile investment for their practices and their patients.
0%
willingness to recommend the Light Adjustable Lens4
0%
would choose the Light Adjustable Lens for themselves, over any other lens4
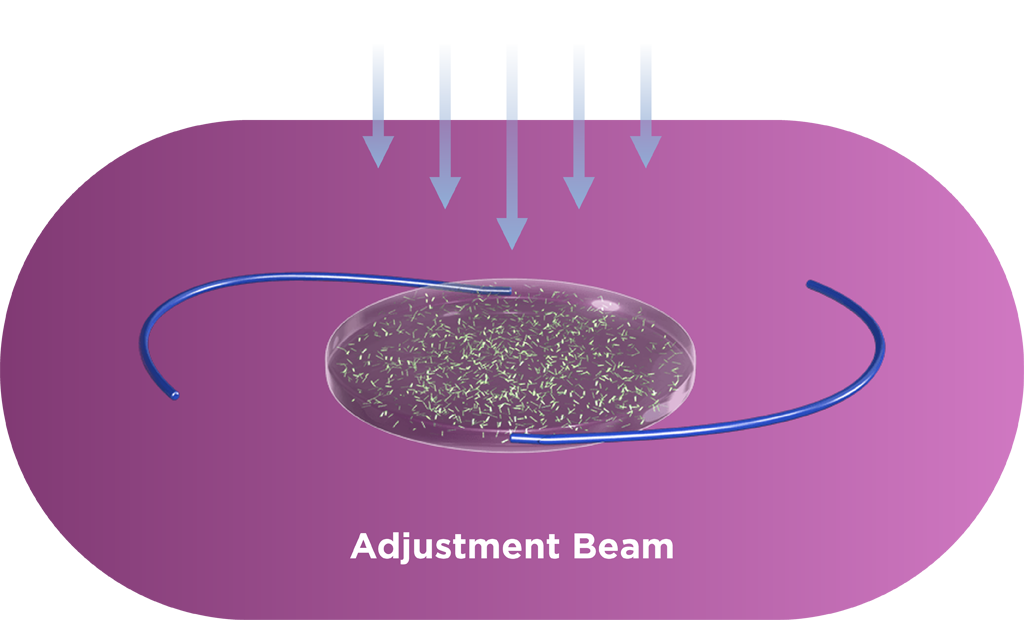
How the Light Adjustable Lens Works
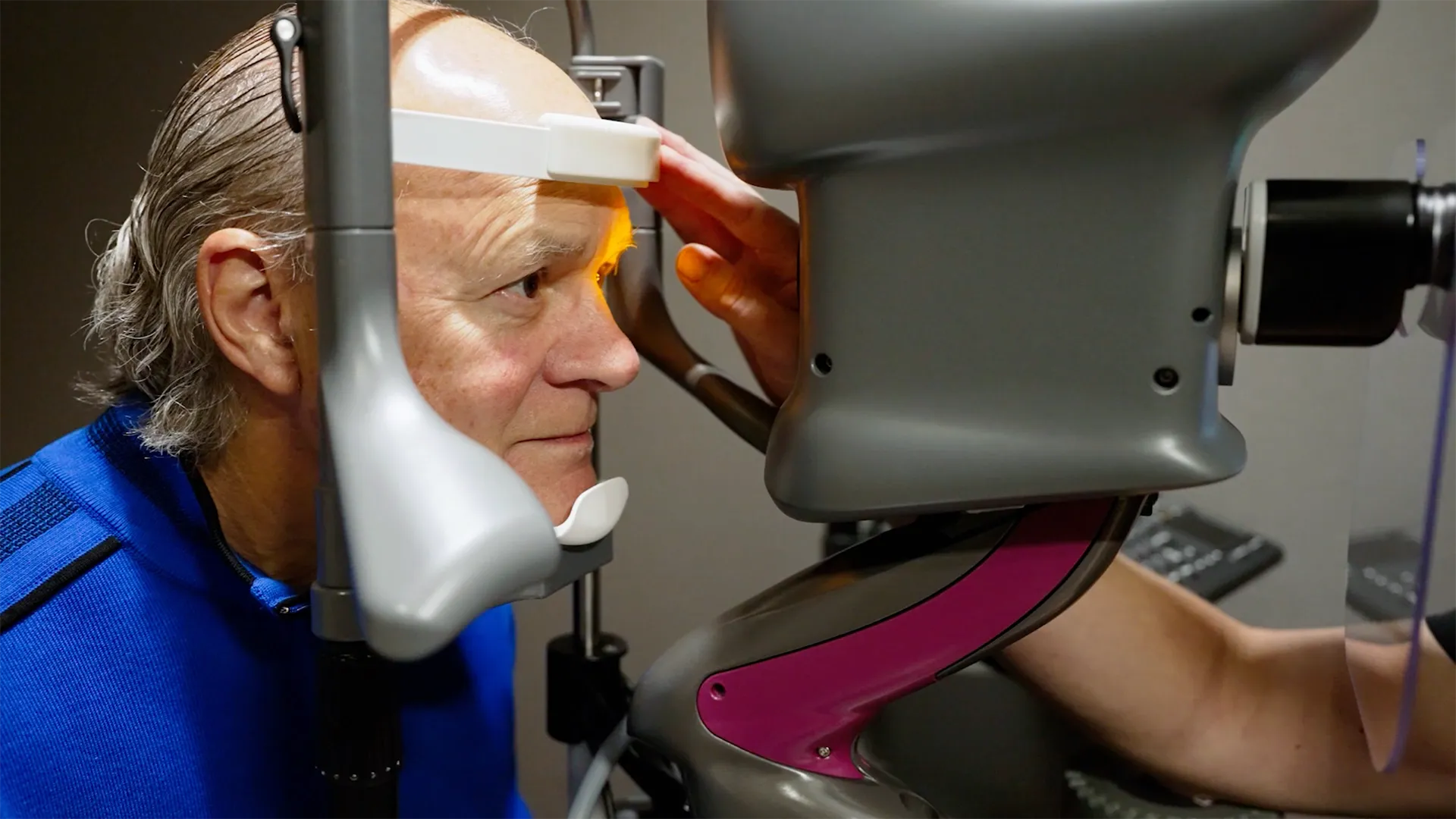
The Light Adjustable Lens is implanted using a standard cataract procedure. Patients then experience their vision and surgeons can adjust the lens over a series of treatments to ensure each patient achieves vision that matches their lives. Each adjustment is an ultraviolet (UV) light treatment performed by the Light Delivery Device™ (LDD™) that corrects refractive error and dials in optimized vision.
Light from the RxSight LDD is directed by the surgeon to the Light Adjustable Lens.
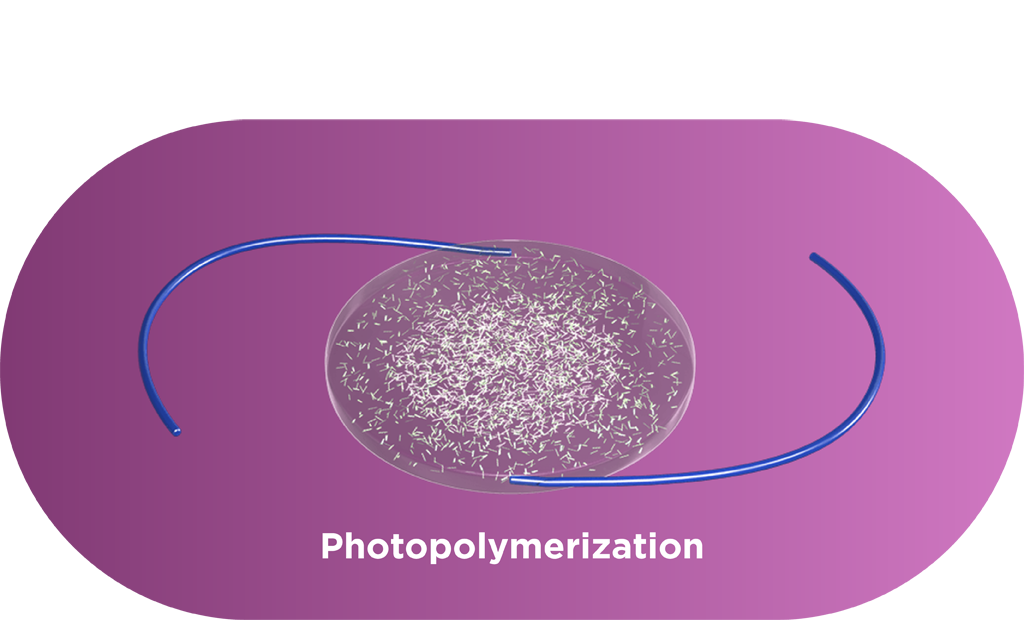
Macromers in the path of the light are photopolymerized.
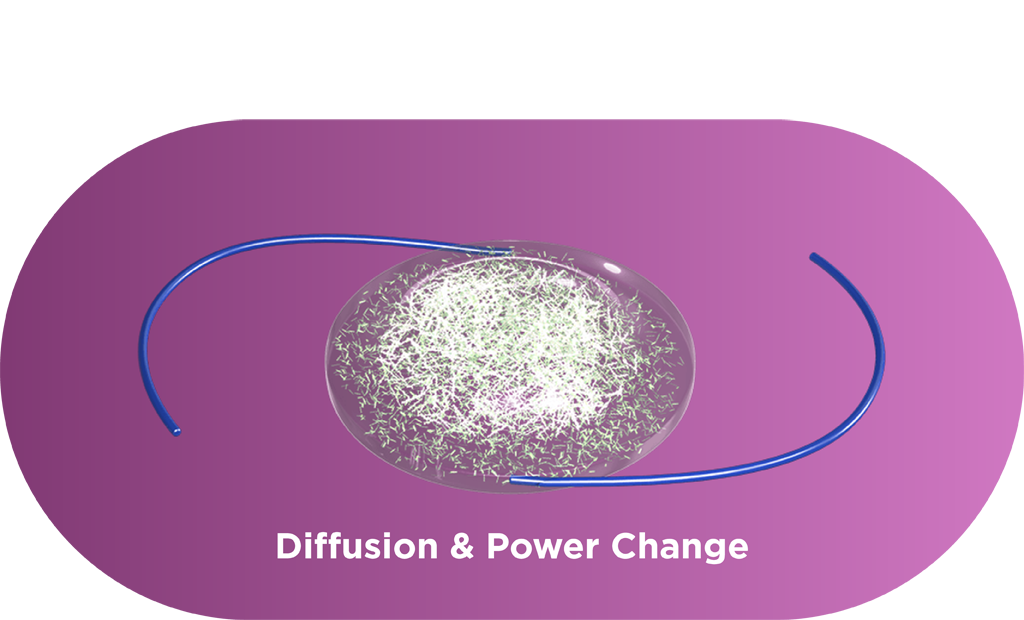
Unpolymerized macromers move into the exposed area, causing precise shape and power change.
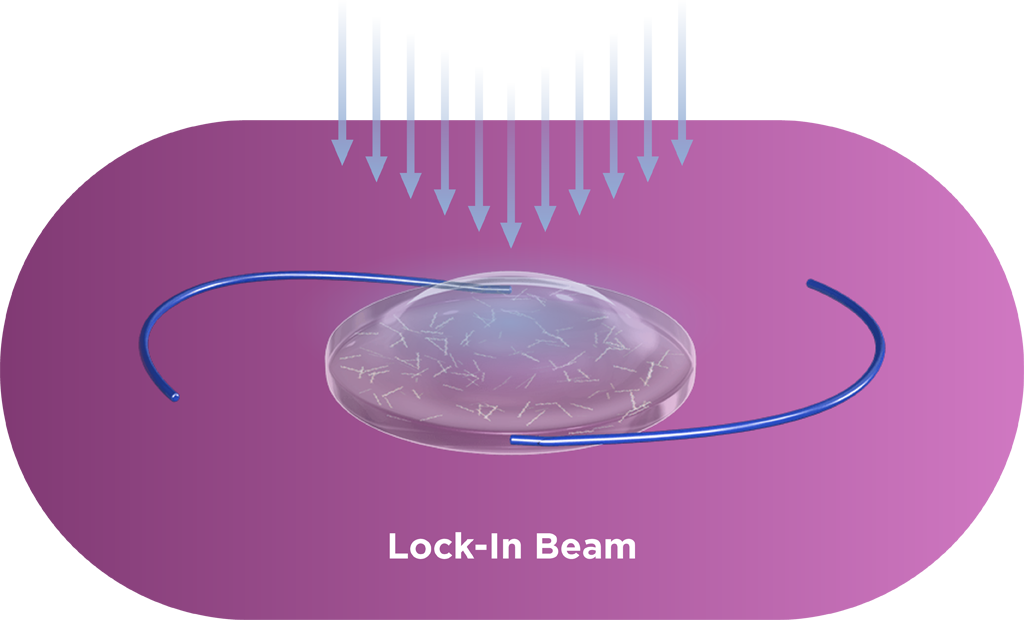
The entire lens is exposed to light to polymerize all the remaining macromers.
The outcome is a precise change in the lens power to match the patient’s individual prescription.
Macromers/polymers are not visible in the lens, and graphic is used only as an illustration.
The Importance of ActivShield™ Technology
ActivShield is a UV protection layer built into the Light Adjustable Lens. Along with the RxSight UV-protective glasses, ActivShield helps prevent accidental sunlight exposure from changing the lens prior to the final lock-in treatment.
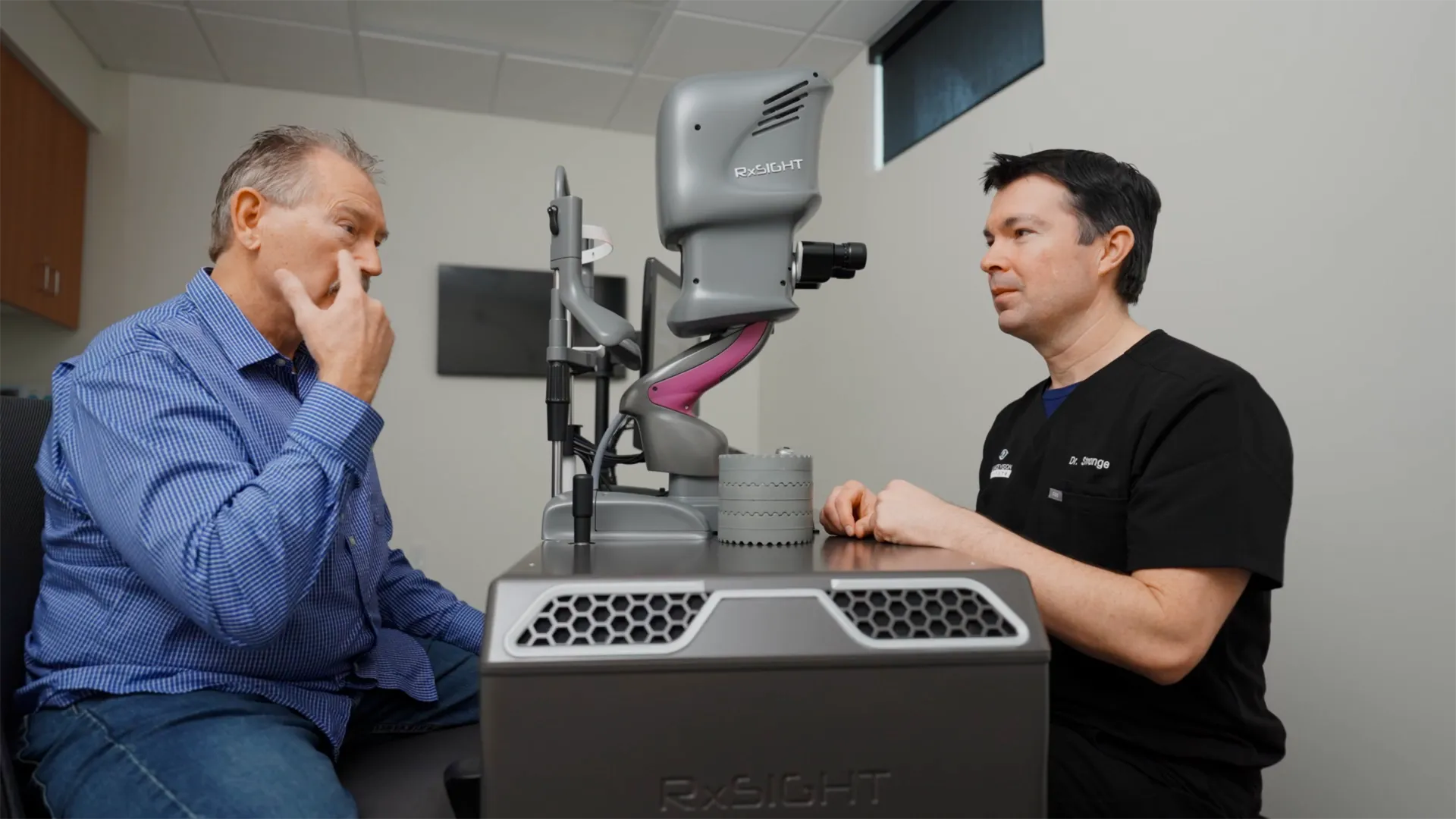
Doctor & Patient Testimonial
Drs. Neda Nikpoor & Mark Bryant
Doctor Testimonial
Dr. Priya Mathews
Patient Testimonial
Andy Corley
Patient Testimonial
Becky Davies
Patient Testimonial
Dr. Jim Davies
Patient Testimonial
Dr. Daniel Durrie
Doctor & Patient Testimonial
Drs. Taylor Strange & David Spivey
Patient Testimonial
Bonnie Whitman
Don’t Get Left in the Dark
Peer Insights. Patient Experience. Practice Performance.
Because every practice is different—and every patient’s vision matters. Let’s explore what’s measurable for your practice. Fill out the form to connect with a specialist and see how this could work for your practice.
Watanabe K, Negishi K, Kawai M, et al. Effect of experimentally induced astigmatism on functional, conventional, and low-contrast visual acuity. J Refract Surg. 2013;29(1):19-24.
RxSight P160055: FDA Summary of Safety and Effectiveness Data. 2017.
Sandoval HP, Donnenfeld ED, Kohnen T, et al. Modern laser in situ keratomileusis outcomes. J Cataract Refract Surg. 2016;42(8):1224-1234.
2025 RxSight Customer Survey.
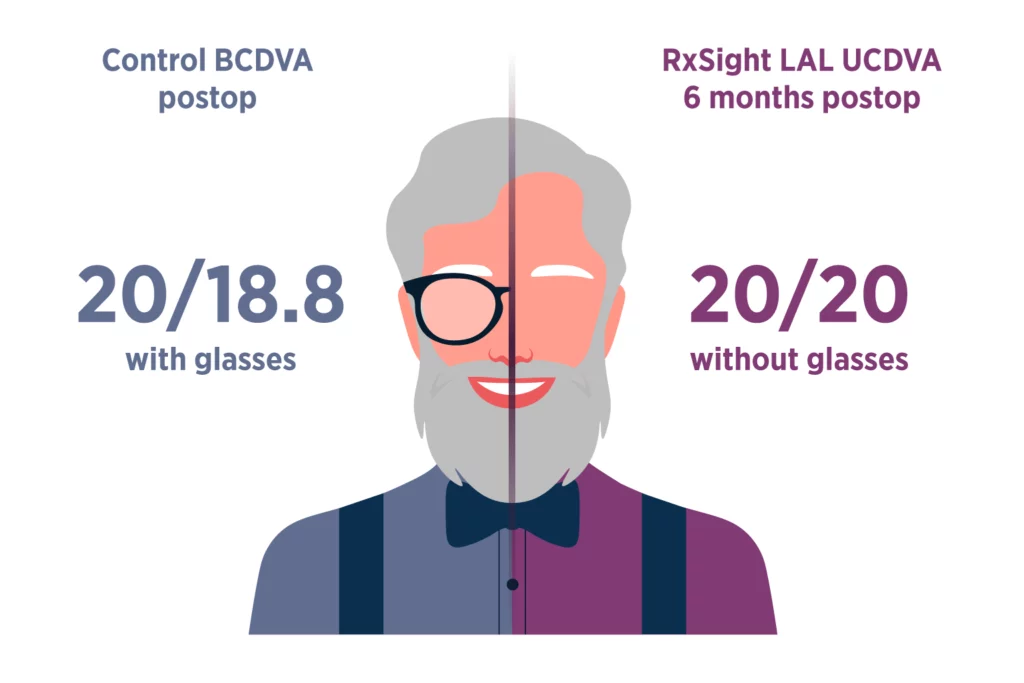
The Light Adjustable Lens provides optimized vision for patient satisfaction.2
Light Adjustable Lens patients saw nearly as well without glasses (UCDVA) as control patients did with glasses (BCDVA).
Since the Light Adjustable Lens is a monofocal lens, there is low risk of dysphotopsias caused by splitting light, leading to potentially enhanced vision and patient satisfaction.
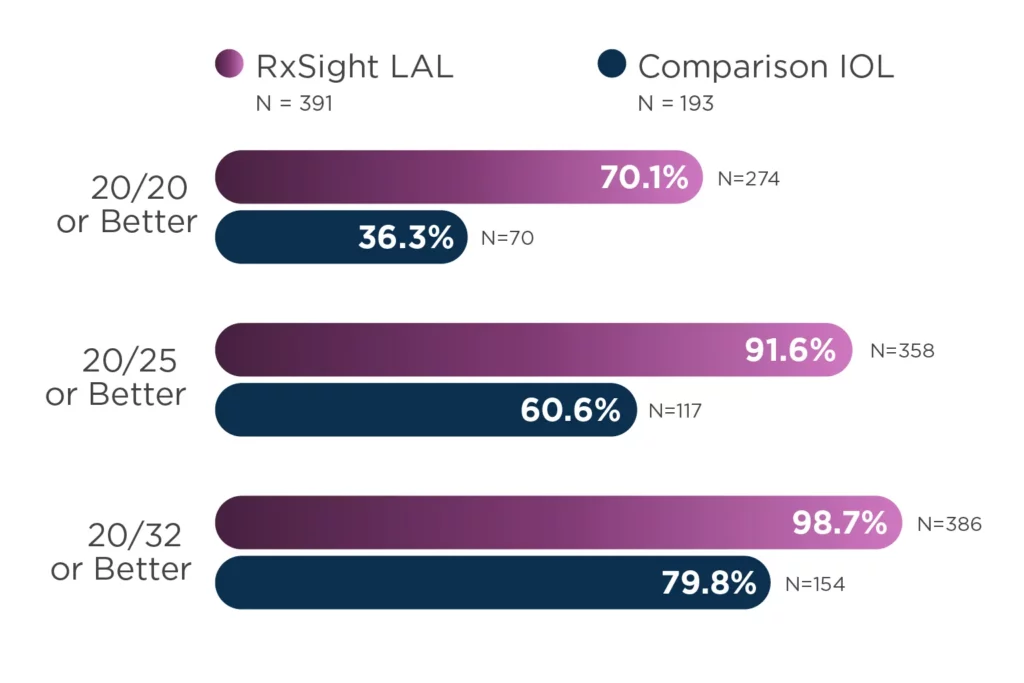
The Light Adjustable Lens offers LASIK-like accuracy in cataract surgery.2,3
92% of eyes (N = 391) achieved results within 0.50 D of target manifest refraction spherical equivalent (MRSE).
Patients are approximately two times more likely to achieve 20/20 vision or better without glasses at 6 months.
The study was a prospective, controlled, multicenter, 12-month study of 600 patients (ITT population) randomized to receive implantation with the RxSight LAL (N = 403) or a commercially available monofocal IOL (N = 197). Effectiveness analyses included 391 LAL patients and 193 control patients. Primary safety variables included best spectacle-corrected visual acuity (BSCVA) at 6 months and incidence of sight-threatening complications and adverse events. Primary effectiveness variables included percent reduction in manifest cylinder at 6 months, percent mean absolute reduction in MRSE at 6 months, and rotation of meridian of LAL at 6 months. Percent of eyes with an uncorrected visual acuity (UCVA) of 20/20 or better at six months post-operatively compared between the LAL treatment group and the monofocal control group was a secondary endpoint.
The Light Adjustable Lens corrects as low as 0.50 D of astigmatism, which is the lowest level approved to be treated.
The ability to treat 0.50 D of postoperative cylinder makes the Light Adjustable Lens the only IOL in the United States approved to correct this level of vision-altering astigmatism.
Astigmatism of as little as 0.50 D can reduce visual acuity by one line, and the impact on dynamic, functional visual acuity and low-contrast acuity is even greater.1